Workshop
Methodology Paper
Kennedy O’Hanley
April 19th
Introduction:
The purpose of this research is to determine if infant mortality in Ethiopia could be decreased if women had to travel less to get to the nearest healthcare facility for post-natal care. Ethiopia does not have a strong health care system. The infant mortality rate is about 39.1 deaths per 1,000 live births. Some women have to travel hours to reach hospitals and healthcare facilities, and because of this distance, are usually unable to make that trip several times after the birth of a child to attend postnatal care. This leads to many infants and children under five dying of preventable infections and diseases. In Ethiopia, 80% of newborn deaths are caused by treatable cases. On the maternal side, mothers are twenty five times more likely to die than mothers from the United States. The infants in Ethiopia are dying not only because of the travel time to adequate healthcare facilities, but also because there is an economic gap dividing the groups of women. This economic gap says that some have the right to necessary resources, and others do not simply because they do not have the money. I have chosen two geospatial methods to consider when looking at the shockingly high infant mortality rates in Ethiopia. Specifically, there have been hazard regressions used in Ethiopia, regarding infant mortality due to travel time. Outside of Ethiopia, there have been several Bayesian models done looking at rates of infant mortality. The Bayesian model I will be looking at today uses demographic variables from the mother. Cox-porportional hazard models have been used to look at several different variables, and eventually reach a conclusion of the true reason so many infants are dying, and the survival rates of infants in many different situations. This is a very good model for this specific topic because we are able to see exactly where the problem lies when dealing with how to efficiently funnel resources into Ethiopia, to improve this problem. My inquiry method would most align with an explanatory inquiry. By looking at the reasoning behind why so many infants are dying in Ethiopia, I am looking at a cause and effect process. Since the resources in Ethiopia are limited and the resources they do have are inadequate, the neonatal and maternal mortality is much higher than it should be.
Method One:
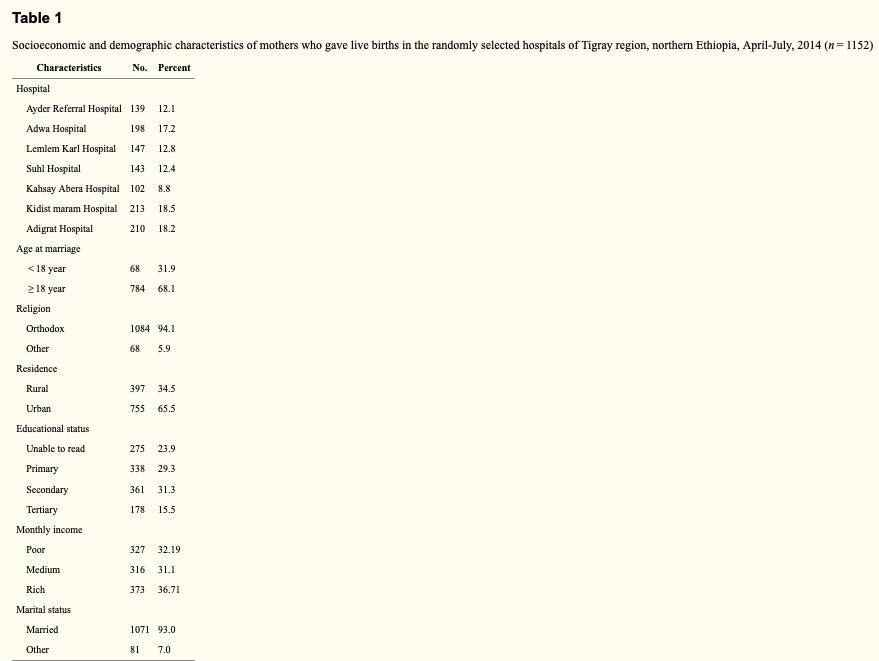
The data in Survival of neonates and predictors of their mortality in Tigray region, Northern Ethiopia: prospective cohort study, is used to determine which covariates trump all others. There are several models and techniques used, and with several variables, and the authors work to investigate which covariate has a higher influence over infant mortality. Distance to the nearest health care facility was among the most dominant independent variables. Along with this, there was data that showed a higher infant mortality rate from those women residing in remote or hard to reach locations, indicating an inadequate amount of resources to all women. The data for this study was processed through STATA version 11.1. The authors used Kaplan-Meier curves to estimate the survival times of the infants. The ultimate goal of the study was to determine the true factors in why the infant mortality rate is so high in Ethiopia, so a Cox-proportional hazard regression model was used to identify these factors. The authors collected their data using a survey. They first created a questionnaire, and then had two trained midwives interview mothers within six hours of giving birth. Mothers and infants were tracked for twenty-eight days: each day they were in the hospital, and then every seven days after that. This ensured that data could be collected at every step of the way. This study had both a spatial and temporal dimension. The authors collected data based on travel time to facilities, where mothers were residing and what conditions they were living in, and the time of death of those infants who did die. There were no variables or covariates that impacted the Cox-proportional hazard regression model negatively or incorrectly.
This model is a very accurate depiction of how Ethiopia’s healthcare system is failing the women of the country greatly. In Survival of neonates and predictors of their mortality in Tigray region, Northern Ethiopia: prospective cohort study, the authors use a Cox-proportional hazard regression to look at survival rates of infants due to travel times. This model is built to analyze travel times, and determine the most influential covariates. The hazard rate models what the effect of the specific variable is. The authors used this data to input many variables and compare them to which infants died. There were many different variables, including travel time to healthcare facilities, home situations, economic need, and more. This model gives a way to determine how long a child will survive for in each condition. It is a useful survival method that helps to accurately narrow in on the death rates that occur with different living situations. In the Cox-proportional hazard model, the authors used lots of variables. Some of which include travel time to facilities, number of children prior to giving birth, number of children mothers were giving birth to (twins, triplets, etc), history of abortion, delivery complications, mode of delivery, and more.
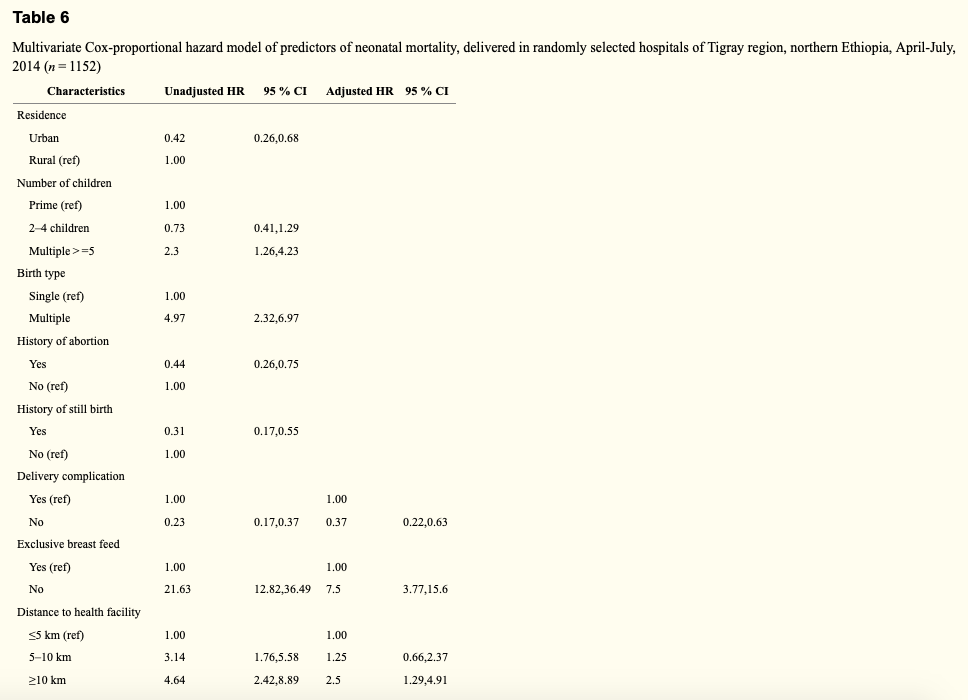 The adjusted HR gives the number of times something is more likely to occur if an infant isn’t given proper care. For instance, if infants were not exclusively breastfed, then they have a 2.5 times higher hazard of death than those babies who were exclusively breastfed. With the Cox-proportional hazard model, there were strong correlations between neonates born from mothers with complications and death, as well as travel time to hospitals and health centers with death. Infants born from mothers with no complications were 63% less likely to die than infants born from mothers with delivery complications. Women who had to travel over ten miles to healthcare facilities gave birth to babies who had a 2.5 times higher chance of dying. The Cox-proportional hazard model determines survival rates. If nothing happens to help improve the lives of these mothers and children, then the model’s survival rates will hold steady. These statistics should give enough of a reason to funnel money into Ethiopia and other countries who need it most, in order to improve upon the healthcare resources.
The adjusted HR gives the number of times something is more likely to occur if an infant isn’t given proper care. For instance, if infants were not exclusively breastfed, then they have a 2.5 times higher hazard of death than those babies who were exclusively breastfed. With the Cox-proportional hazard model, there were strong correlations between neonates born from mothers with complications and death, as well as travel time to hospitals and health centers with death. Infants born from mothers with no complications were 63% less likely to die than infants born from mothers with delivery complications. Women who had to travel over ten miles to healthcare facilities gave birth to babies who had a 2.5 times higher chance of dying. The Cox-proportional hazard model determines survival rates. If nothing happens to help improve the lives of these mothers and children, then the model’s survival rates will hold steady. These statistics should give enough of a reason to funnel money into Ethiopia and other countries who need it most, in order to improve upon the healthcare resources.
Method two:
In Bayesian Hierarchical Modeling of Infant Mortality in Nigeria, the data collected was put into several different bayesian models, and was mainly used to determine the geographical aspects of the women and situations. Afterward, the authors included several boxplots charting infant death rates to show what they had discovered. The authors used data from Multiple Indicator Cluster Survey. This data was processed by Statistical Package for Social Scientists (SPSS) software, Version 21. The data was then put into bayesian models for testing in this specific study. The data in this study was taken from a Multiple Indicator Cluster Survey held in Nigeria. This data includes specifics about women and children, in order to attempt to improve the women and children’s lives. This data was collected by the National Bureau of Statistics (NBS), the National Primary Health Care Development Agency (NPHCDA), and the National Agency for the Control of Aids (NACA). This study looks specifically at the 34, 376 women and the 28,085 mothers of children under five. This data just has a spatial dimension. Each variable included is either categorized as a demographic or a socioeconomic aspect. Since there is no measurement that deals with time, and only measurements dealing with what a woman’s life looks like, it does not have a temporal dimension. The validity of the data was checked using four different statistical tools: standard error, coefficient of variation, design effect and confidence intervals. Because of this, the data has been thoroughly checked for mistakes and is reliable.
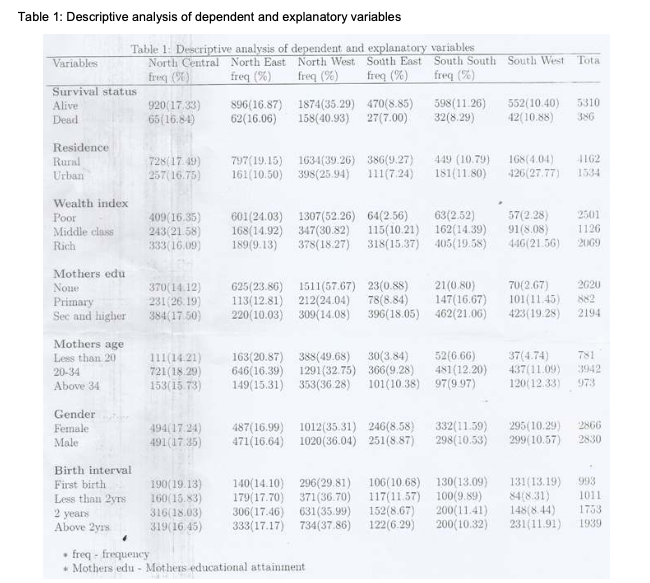
In Bayesian Hierarchical Modeling of Infant Mortality in Nigeria, the authors use a Baysian model to look at the influences of infant mortality. There were two bayesian models used. The first one was a single-level bayesian logistic regression model. The individual variables were used as the predictors, and does not look at anything that could be negatively impacting the study. The second model adds in the geographics of the places the infants were born, in order to know if state and region of birth have an effect of infant mortality. The second model measures the probability that children living in the same areas are exposed to the same conditions. The authors used their individual variables and regions from which each mother resides, to determine if there was a correlation between the state where the mother lives and the condition of the infant. The authors used specifically the individual variables in the first model, in order to learn the probability of an infant dying before they reach one year. The second model included the regions in which the mothers reside. This was a bayesian hierarchical logistics model, which factors in spatial data. In the bayesian hierarchical logistics model, there are two kinds of variables used. There are the variables assigned to the demographics and socioeconomic status of the mother, such as economic status, education of mother, mother’s age, gender and previous children. There are also variables assigned to the region and area that the mothers live. The first set of variables is used for the first, and more simple bayesian model, while the second model is a hierarchical model, which includes the second set of variables as well.
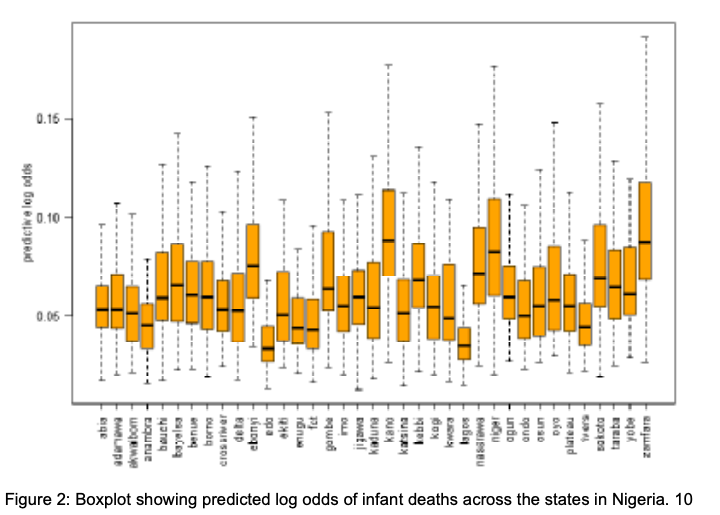
These boxplots are showing the diversity in the results from the bayesian model. It is easy to see that the different places in Nigeria vary greatly in their probability of infant mortality. The difference in infant mortality between Kano, Nigeria and Lagos, Nigeria. This study found that type of residence, child’s gender, and number of children were significant determinants of infant mortality. The estimates showed that living in an urban area decreases an infant’s chance of dying greatly compared to those infants residing in a rural area. This is most likely because those in urban areas have easier and faster access to resources. The bayesian hierarchical model determines odd ratios, so much like the Cox-proportional hazard model, it’s ratio will hold if nothing is done to help the women and children of Nigeria.

Conclusion:
I do not believe one is better than the other. Both models essentially measure the same thing, with the same variables. They just give a different output. There are already Cox-proportional hazard models in Ethiopia, so it would be beneficial to get more bayesian models using the data for Ethiopia, in order to get a clearer picture of the horrors that pregnant women are having to face there. These two methods are complementary, considering they both have the same end goal: to determine whether travel time to healthcare facilities has an impact on infant mortality. While one method looks at and determines the survival rate, the other looks at the odds that the infants will die. Both of these studies are looking at the opposite side of this statistic.
There are currently no bayesian models done in Ethiopia. I believe that using new, improved models would help contribute more evidence as to why Ethiopia’s healthcare system needs to be greatly improved. My research question, to determine if infant mortality in Ethiopia could be decreased, if women had to travel less to get to the nearest healthcare facility for post-natal care, was mostly answered by these two models. Yes. The time it takes to travel to healthcare facilities does have an effect on infant mortality, and for that matter, a great impact. By funneling in money, resources, and new healthcare facilities and hospitals, infant mortality would decrease because women wouldn’t have to travel so far to safely give birth. Ethiopian women should not have to go through the pain of losing a child simply because their country does not have the resources to take care of it’s people. Too many infants are dying in Ethiopia, and also all around the world. This could be stopped if we allocate the correct amount of resources to areas that need it. In order to truly lessen the infant mortality rate, travel time for women must be decreased.
Bibliography:
Alaba, Oluwayemisi Oyeronke, and Chidinma Godwin. “Bayesian Hierarchical Modeling of Infant Mortality in Nigeria.” Global Journal of Pure and Applied Sciences, vol. 25, no. 2, 2019, p. 175., doi:10.4314/gjpas.v25i2.7.
Alegana, V. A., Atkinson, P. M., Pezzulo, C., Sorichetta, A., Weiss, D., Bird, T., … Tatem, A. J. (2015). Fine resolution mapping of population age-structures for health and development applications. Journal of The Royal Society Interface, 12(105), 20150073. doi: 10.1098/rsif.2015.0073
Bailey, P. E., Keyes, E. B., Parker, C., Abdullah, M., Kebede, H., & Freedman, L. (2011). Using a GIS to model interventions to strengthen the emergency referral system for maternal and newborn health in Ethiopia. International Journal of Gynecology & Obstetrics, 115(3), 300–309. doi: 10.1016/j.ijgo.2011.09.004
Dadi, Lelisa Sena, et al. “Maternal and Newborn Health Services Utilization in Jimma Zone, Southwest Ethiopia: a Community Based Cross-Sectional Study.” BMC Pregnancy and Childbirth, vol. 19, no. 1, 2019, doi:10.1186/s12884-019-2335-2. Ebener, S., Guerra-Arias, M., Campbell, J., Tatem, A. J., Moran, A. C., Johnson, F. A., … Matthews, Z. (2015). The geography of maternal and newborn health: the state of the art. International Journal of Health Geographics, 14(1). doi: 10.1186/s12942-015-0012-x
Mcpadden, J., Durant, T. J., Bunch, D. R., Coppi, A., Price, N., Rodgerson, K., … Schulz, W. L. (2019). Health Care and Precision Medicine Research: Analysis of a Scalable Data Science Platform. Journal of Medical Internet Research, 21(4). doi: 10.2196/13043
Mengesha, Hayelom Gebrekirstos, and Berhe W. Sahle. “Cause of Neonatal Deaths in Northern Ethiopia: a Prospective Cohort Study.” BMC Public Health, vol. 17, no. 1, 2017, doi:10.1186/s12889-016-3979-8.
Okwaraji, Y, et al. “PS53 Effect Of Geographical Access To Health Facilities On Child Mortality In Rural Ethiopia: A Community Based Cross Sectional Study.” Journal of Epidemiology and Community Health, vol. 66, no. Suppl 1, 12 Mar. 2012, doi:10.1136/jech-2012-201753.152. Sahle, Geletaw. “Ethiopic Maternal Care Data Mining: Discovering the Factors That Affect Postnatal Care Visit in Ethiopia.” Health Information Science and Systems, vol. 4, no. 1, 2016, doi:10.1186/s13755-016-0017-2.
Tatem, A. J., Campbell, J., Guerra-Arias, M., Bernis, L. D., Moran, A., & Matthews, Z. (2014). Mapping for maternal and newborn health: the distributions of women of childbearing age, pregnancies and births. International Journal of Health Geographics, 13(1), 2. doi: 10.1186/1476-072x-13-2
Tekelab, Tesfalidet, et al. “Neonatal Mortality in Ethiopia: a Protocol for Systematic Review and Meta-Analysis.” Systematic Reviews, vol. 8, no. 1, 2019, doi:10.1186/s13643-019-1012-x.